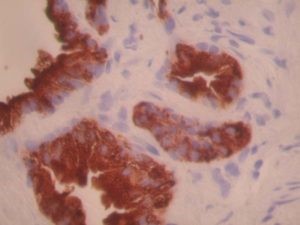
Prostatic acid phosphatase by IHC
Prostatic acid phosphatase by IHC-12376 - Technical only, 12379 - Technical & interpretation
LAB12379
- All IHC stains will include a positive control tissue
PSAP is fairly specific for prostate tissue
- Immunoreactivity for PSAP (and PSA) is generally more intense and homogeneous in benign prostate tissue than in prostatic carcinoma. Occasional cases of prostatic squamous metaplasia may show focal reactivity
- Other normal/non-neoplastic tissues with reported PSAP reactivity:
- periurethral glands*
- anal glands (male only)*
- urachal remnants*
- renal tubules
- neutrophils (cross reactivity with leukocyte acid phosphatase)
- pancreatic islet cells
- neuroendocrine cells in clonic crypts
- seminal vesicle**
- cystitis cystica and glandularis*
- (rare reports of focal PSAP reactivity in hepatocytes, breast ducts, and gastric parietal cells) - Other neoplasms with reported PSAP reactivity:
- pure adenocarcinoma of the bladder*
- periurethral gland carcinomas*
- gastrointestinal carcinoids (approx. 70% of rectal carcinoids; the frequency of PAP positivity decreases as one ascends the gastrointestinal tract)
- pancreatic islet cell tumors
- (rare reports of PSAP reactivity in renal cell carcinoma and breast carcinoma) - In general, any cloacal derived tissue may show reactivity with PSAP
- Normal and neoplastic transitional epithelium is negative
Carcinoids found within the ovary, kidney, breast, liver, and head and neck have been PSAP negative
*both PSAP and PSA reactivity are reported
**reported for antibodies developed against seminal fluid.
Note:
PSAP monoclonal antibodies have shown a lower sensitivity compared to polyclonal antiserum (In two studies of poorly differentiated prostate carcinoma, monoclonal antibodies stained 59% and 60% of cases whereas polyclonal antibodies stained 83% and 86% of cases).
Submit a formalin-fixed, paraffin embedded tissue block
Formalin-fixed, paraffin embedded (FFPE) tissue block
FFPE tissue section mounted on a charged, unstained slide
Ambient (preferred)
- Unlabeled/mislabeled block
- Insufficient tissue
- Slides broken beyond repair
Immunohistochemical staining and microscopic examination
If requested, an interpretive report will be provided
Specifications
- Monoclonal antibody directed against prostatic acid phosphatase
Staining pattern
- Cytoplasmic based staining; prostatic acinar and ductal epithelium reactivity tends to concentrate in the apical portion. Reactivity is also present in prostatic secretions and on the surface of corpora amylacea
References
- Epstein JI. PSA and PSAP as immunohistochemical markers in prostate cancer. Urologic Clinics of North America 1993; 20(4):757-70.
- Ro JY, et al. Small cell carcinoma of the prostate: immunohistochemical and electron microscopic study of 18 cases. Cancer 1987; 59:977-82.
- Azumi. Prostatic acid phosphatase in carcinoid tumors. Am J Surg. Pathol 15(8):785-790, 1991.
88341 - each additional stain